Every January, general surgery residents walk into their testing centers exhausted. They have spent the last four months trying to read huge textbooks between cases, or they clicked through contradicting question banks while fighting fatigue. This sort of passive studying yields mediocre results.
To dominate the 2027 American Board of Surgery In-Training Examination (ABSITE), residents must abandon these outdated methods. The master educators behind SurgBoards have spent over a decade analyzing how trainees actually retain information under extreme time constraints. The conclusion is absolute. Active recall is the only strategy that guarantees success.
Attending Pearl
“Passive reading creates a false sense of fluency. Recognizing a concept on a page does not mean the brain can retrieve that information when a complex clinical vignette is presented under a strict time limit.”
The Trap of Passive Reading
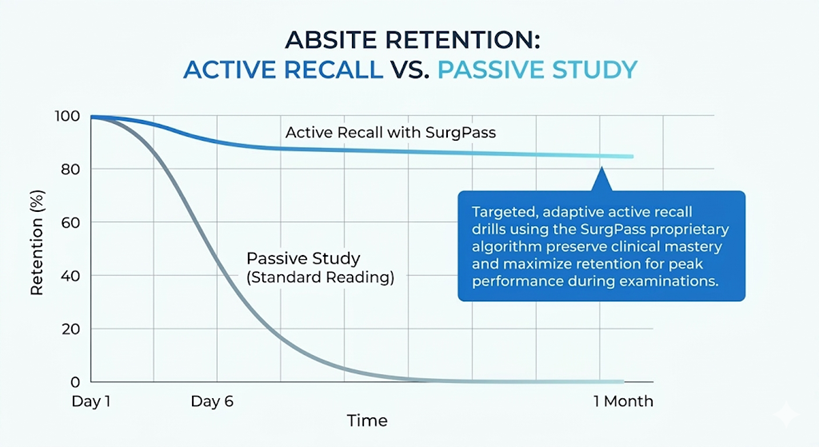
The most common mistake a surgical resident makes is attempting to read standard surgical atlases cover to cover. While it’s nice to have read one of the “main textbooks”, the reality is there are patients to see, boards to study for, operations to prepare for, attendings to appease, and a life to live! For a lot of residents, passive reading creates a false sense of fluency. Recognizing a concept on a page or a flashcard does not mean the brain can retrieve that information when a complex clinical vignette is presented under a time limit.
Furthermore, surgical trainees simply do not have the hours required for passive review. An unpredictable call schedule and heavy trauma rotations demand a study method that maximizes every available minute. This is exactly why SurgPass was engineered entirely around active concept retention rather than passive consumption.
Strategic Timing for the 2026-2027 Exam
The traditional ABSITE testing window occurs in late January and early February. Preparing for the ABSITE requires a strategic ramp-up period rather than a frantic cram session. Follow this proven pacing strategy to peak exactly on test day:
The Power of Targeted Active Recall
Rather than building manual flashcards that eat up your limited free time, use an automated system like SurgPass that works quietly in the background. When you miss a question in the main QBank, the adaptive engine automatically unlocks targeted SurgHits. These are smaller, bite-sized multiple-choice questions that test the specific micro-concepts of the parent question you got wrong.
This process never interrupts your study flow. SurgHits do not pop up immediately after a missed question to hijack your session. Instead, they are saved to a separate spaced-repetition portal. You can grind through QBank questions all day and choose to tackle your accumulated SurgHits tomorrow, next week, or whenever you want. You are completely in control of your schedule.
When you are ready, these active recall drills resurface the exact board-relevant pearls you need to review. This forces your brain to retrieve the information repeatedly, building the neural pathways required to recall data under pressure without you needing to spend time typing notes or deciding on the fly what needs a “refresher”. Plus, because the content is exclusively human-authored by master surgical educators, every SurgHits reflects the realistic concepts that board examiners actually test.
Handling Interruptions Without the Penalty
The greatest threat to a long-term study plan is the inevitable heavy clinical rotation. Traditional spaced repetition systems punish trainees for missing days, creating a large backlog of hundreds of due items.
The SurgPass algorithm is designed specifically for the unpredictable realities of surgical residency. If a trainee is unable to log in for three weeks due to an intense ICU month, the system intelligently adapts. Progress pauses seamlessly without generating a penalty backlog. When the resident returns, the algorithm picks up exactly where it left off, preventing study fatigue.
Crunch Time and Turbo Mode
In the final weeks leading up to the ABSITE exam, studying must become highly aggressive. Reading new material is no longer the most effective method. This is the exact moment to activate Turbo Mode on the SurgPass platform. This specialized feature accelerates the algorithm, rapidly resurfacing missed concepts and high-yield SurgHits to guarantee peak retention immediately prior to test day.
Coupled with a testing interface that perfectly mirrors the actual Prometric ABS ABITE exam, residents can walk into test day with absolute confidence, having built genuine clinical mastery rather than just passing familiarity.
The Ultimate ABSITE FAQ: Logistics, Dates & Scoring
When is the ABSITE administered?
The exam is offered annually during a specific testing window between late January and early February. Your residency program will select the exact day or days within this window to administer the exam to all residents.
How do I register and how much does it cost?
You do not register or pay for the ABSITE individually. The American Board of Surgery provides the exam directly to all ACGME-accredited general surgery residency programs. Your program director and coordinator are responsible for ordering the exam in the fall, submitting the trainee roster, and covering all associated exam fees. The ABS does not accept individual registrations or payments from residents.
How long is the exam and how many questions are there?
The ABSITE consists of approximately 250 multiple-choice questions. You are given a total of five hours to complete the test, which is administered in two 2.5-hour blocks with a scheduled break in between. This strict time limit means you have just over one minute per question, which is exactly why rapid pattern recognition and active recall are so important.
Where do I take the test?
Unlike the ABS Qualifying or Certifying exams, the ABSITE is not taken at a Pearson VUE testing center. It is administered entirely online as a live, in-person, proctored exam using your residency program’s own computer facilities (typically a reserved conference room, computer lab, or library at your hospital).
When do I get my ABSITE results?
Results are not available immediately upon finishing the test. The ABS compiles and releases the scoring reports to program directors typically in late February or early March. Your program director or coordinator will then distribute your individual score report to you. The ABS does not retain copies or send transcripts directly to residents, so be sure to save your report!
Why did the ABS stop reporting percentiles?
In January 2025, the American Board of Surgery officially discontinued percentile scores. Because resident scores clustered so tightly in the middle of the bell curve, a difference of just one or two correct questions could swing a resident’s percentile by 10 to 20 points. This mathematical quirk created unnecessary anxiety and made percentiles an imprecise metric for high-stakes decisions like fellowship selection. Today, the ABS only reports your “Percent Correct” and a “Standard Score.”
What is considered a good Percent Correct?
Because the ABSITE is the exact same 250-question test for every resident from intern to chief, your target percent correct should generally increase as you progress through training. While the national averages fluctuate slightly each year depending on the test’s difficulty, here is a general benchmark for where most residents fall:
- PGY 1 & PGY 2: 60% to 65% correct. You are establishing your foundational knowledge.
- PGY 3 & PGY 4: 68% to 72% correct. You are refining your clinical judgment and operative management.
- PGY 5 (Chiefs): 75% or higher. You are proving you have the mastery required to pass the written boards.
Scoring consistently in the high 70s or 80s at any level is considered an exceptional, top-tier performance.
Am I graded against everyone or just my class?
Your “Percent Correct” is simply the raw, objective number of questions you answered correctly out of the total. However, the ABS also provides a “Standard Score” alongside it. This standard score is set to a mean of 500 with a standard deviation of 100, and it strictly compares you against other residents at your exact PGY level. An intern is never penalized for not knowing as much as a chief. The ultimate goal is to demonstrate steady, year-over-year growth.